
Americans' Access to Medical Care Deteriorates Between 2003 and 2007 |
||
Trends in Americans' Access to Needed Medical Care, 2001-2003 Tracking Report No. 10 |
||
Mixed Signals: Trends in Americans' Access to Medical Care, 2007-2010 Tracking Report No. 25 |
||
Falling Behind: Americans' Access to Medical Care Deteriorates, 2003-2007
Tracking Report No. 19
June 2008
Peter J. Cunningham, Laurie E. Felland
The number and proportion of Americans reporting going without or delaying needed medical care increased sharply between 2003 and 2007, according to findings from the Center for Studying Health System Change’s (HSC) nationally representative 2007 Health Tracking Household Survey. One in five Americans—59 million people—reported not getting or delaying needed medical care in 2007, up from one in seven—36 million people—in 2003. While access deteriorated for both insured and uninsured people, insured people experienced a larger relative increase in access problems compared with uninsured people. Moreover, access declined more for people in fair or poor health than for healthier people. In addition, unmet medical needs increased for low-income children, reversing earlier trends and widening the access gap with higher-income children. People reporting access problems increasingly cited cost as an obstacle to needed care, along with rising rates of health plan and health system barriers.
- Access to Needed Medical Care Declines
- Access Deteriorates for Insured and Uninsured
- Sickest Face More Access Problems
- Children’s Access Decreases
- Cost Concerns Intensify
- More Health System and Plan Barriers
- Implications
- Notes
- Data Source
- Supplementary Tables
Access to Needed Medical Care Declines
![]() n 2007, approximately 20 percent of the U.S. population—one
in five people—reported not getting or delaying needed medical care at
some point in the previous 12 months, up significantly from 14 percent—one
in seven—in 2003. The dramatic decline in access between 2003 and 2007
signals a sharp change in Americans’ access to care, which was relatively stable
between 1997 and 2003, including some gains.1 Increased
health care costs, along with health insurance-related and health system-related
problems, appear to be the major contributor to Americans’ declining access
to care.
n 2007, approximately 20 percent of the U.S. population—one
in five people—reported not getting or delaying needed medical care at
some point in the previous 12 months, up significantly from 14 percent—one
in seven—in 2003. The dramatic decline in access between 2003 and 2007
signals a sharp change in Americans’ access to care, which was relatively stable
between 1997 and 2003, including some gains.1 Increased
health care costs, along with health insurance-related and health system-related
problems, appear to be the major contributor to Americans’ declining access
to care.
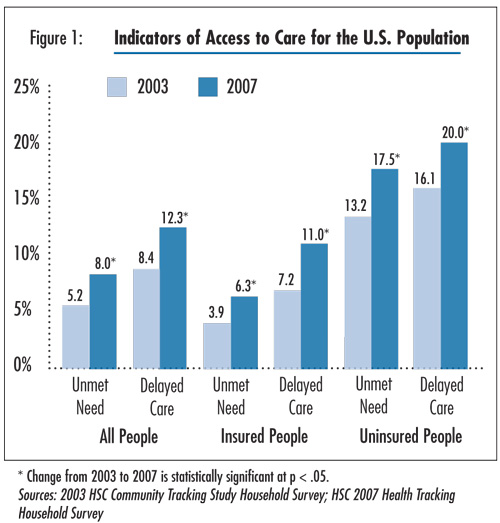
In 2007, more than 23 million people reported going without needed care and approximately 36 million people delayed seeking care, for a total of 59 million people reporting access problems, according to findings from HSC’s nationally representative 2007 Health Tracking Household Survey (see Data Source). The proportion of Americans reporting unmet needs increased by 2.8 percentage points between 2003 and 2007 (5.2% vs. 8%), the equivalent of about 9.5 million more people going without medical care (see Figure 1 and Supplementary Table 1). The proportion of Americans delaying needed care increased by 3.9 percentage points between 2003 and 2007 (8.4% vs. 12.3%), the equivalent of 13.5 million more people.
Click here to view this figure as a PowerPoint slide.
Access Deteriorates for Insured and Uninsured
![]() ninsured people continue to have much higher levels of
unmet medical need and delayed care compared with insured people, and access
for the uninsured decreased between 2003 and 2007 for both uninsured people
with incomes below 200 percent of poverty—$41,300 for a family of four
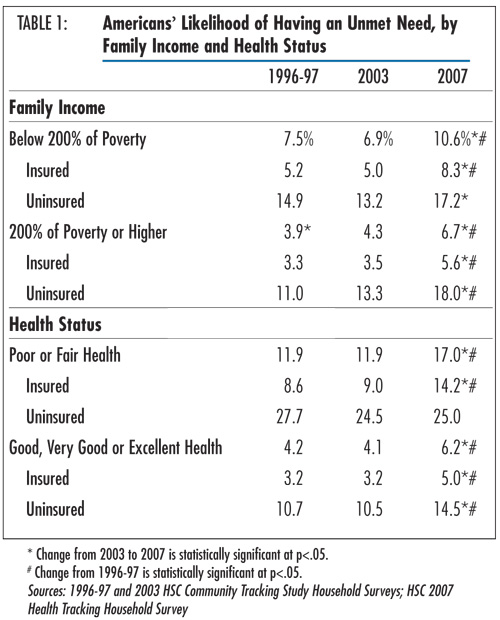
in 2007—and above (see Table 1). These findings are
consistent with other HSC research showing declines in physician charity care
and strained safety net capacity to serve uninsured persons resulting from financial
and competitive pressures in health care markets.2
ninsured people continue to have much higher levels of
unmet medical need and delayed care compared with insured people, and access
for the uninsured decreased between 2003 and 2007 for both uninsured people
with incomes below 200 percent of poverty—$41,300 for a family of four
in 2007—and above (see Table 1). These findings are
consistent with other HSC research showing declines in physician charity care
and strained safety net capacity to serve uninsured persons resulting from financial
and competitive pressures in health care markets.2
However, insured people also faced large increases in unmet need between 2003 and 2007. In fact, insured people experienced a greater percentage increase in unmet medical needs compared with uninsured people—a 62 percent increase for the insured vs. a 33 percent increase for the uninsured. As a result, ironically, the access gap between insured and uninsured people narrowed slightly. In 2003, uninsured people were 3.4 times as likely to report going without care as insured people and 2.8 times as likely in 2007. Also, increases in unmet need were relatively consistent across both low- and high-income insured groups. Rising out-of-pocket costs in the form of higher deductibles, coinsurance and copayments likely account for much of the increased unmet need among insured people.3 Other HSC research confirms that insured people with greater out-of-pocket medical costs are more likely to delay or go without needed care.4
Back to Top
Click here to view this figure as a PowerPoint slide.
Sickest Face More Access Problems
![]() nmet medical needs are greater for people in poor or fair health compared with people in good, very good or excellent health. Sicker people use more health care and, therefore, have more chances to encounter obstacles in getting care. However, access to care worsened the most for people in poor or fair health, a particular concern because sicker people are in greater need of care. Overall, people in poor or fair health with an unmet need increased by 5.1 percentage points between 2003 and 2007 (11.9% vs. 17.0%), compared with an increase of 2.1 percentage points for people in good, very good or excellent health (4.1% vs. 6.2%).
nmet medical needs are greater for people in poor or fair health compared with people in good, very good or excellent health. Sicker people use more health care and, therefore, have more chances to encounter obstacles in getting care. However, access to care worsened the most for people in poor or fair health, a particular concern because sicker people are in greater need of care. Overall, people in poor or fair health with an unmet need increased by 5.1 percentage points between 2003 and 2007 (11.9% vs. 17.0%), compared with an increase of 2.1 percentage points for people in good, very good or excellent health (4.1% vs. 6.2%).
Insured people in poor or fair health experienced more than a 5 percentage point increase in unmet need (9.0% in 2003 vs. 14.2% in 2007), while insured people in good, very good or excellent health experienced a somewhat smaller increase of 1.8 percentage points (3.2% in 2003 vs. 5% in 2007). Uninsured people in poor or fair health reported the greatest access problems among all people in fair or poor health, with one in four reporting in 2007 that they went without needed care.
Back to Top
Children’s Access Declines
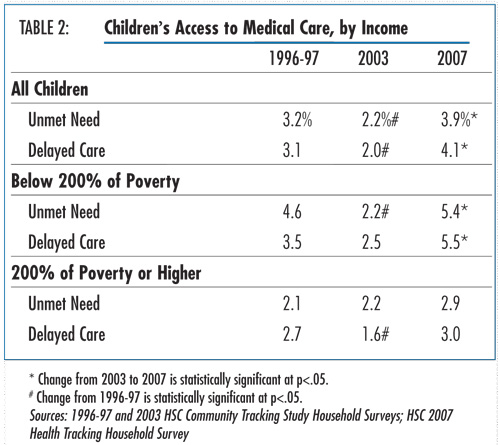
![]() s the overall U.S. population experienced increases in
unmet need and delayed care between 2003 and 2007, children were no exception
(see Table 2). Low-income children encountered the greatest
increase in unmet needs among all children, reversing the gains they experienced
between 1997 and 2003. As a consequence, income differences in unmet need for
children were eliminated by 2003, but these disparities returned by 2007.
s the overall U.S. population experienced increases in
unmet need and delayed care between 2003 and 2007, children were no exception
(see Table 2). Low-income children encountered the greatest
increase in unmet needs among all children, reversing the gains they experienced
between 1997 and 2003. As a consequence, income differences in unmet need for
children were eliminated by 2003, but these disparities returned by 2007.
While gains in access among low-income children between 1997 and 2003 likely reflect expansions in Medicaid and the State Children’s Health Insurance Program (SCHIP) that reduced the number of uninsured children, Medicaid and SCHIP enrollment among low-income children has remained largely unchanged since 2003. Restrictions on eligibility and enrollment policies by some states, as well as new federal requirements for Medicaid applicants to document citizenship, may have contributed to the lack of growth in Medicaid and SCHIP enrollment since 2003.5 At the same time, continued decreases in employer-sponsored coverage have increased the proportion of low-income children who are uninsured (findings not shown). In addition, factors affecting the general population’s access to care—cost concerns and health plan and health system barriers—likely contributed to increased access problems for children.
Back to Top
Click here to view this figure as a PowerPoint slide.
Cost Concerns Intensify
![]() or the 59 million people reporting an access problem, cost
was the most frequently cited—and a growing—obstacle to care. In 2007, 69 percent
of people who went without or delayed needed care cited worries about cost,
a 3.8 percentage point increase from 2003 (see Supplementary
Table 2).
or the 59 million people reporting an access problem, cost
was the most frequently cited—and a growing—obstacle to care. In 2007, 69 percent
of people who went without or delayed needed care cited worries about cost,
a 3.8 percentage point increase from 2003 (see Supplementary
Table 2).
While cost continued to be the overwhelming concern among uninsured people (more than 90% of uninsured people reported cost as a barrier across all three surveys), the increase in cost barriers occurred mostly among insured people. As mentioned earlier, higher patient cost sharing—people facing higher deductibles and other increased out-of-pocket expenses for medical services—likely is driving growing cost concerns among insured people. As the underlying cost of medical services and insurance premiums have increased, many employers have reduced benefits and increased patient cost sharing through so-called benefit buy-downs as a way to moderate large premium increases and pass along more of the cost increases to employees.6
Back to Top
More Health System and Plan Barriers
![]() fter concerns about costs, health system-related concerns were the next most frequently cited reason for access problems, followed by health plan-related issues. Both health system and health plan barriers to care jumped approximately 9 percentage points between 2003 and 2007.
fter concerns about costs, health system-related concerns were the next most frequently cited reason for access problems, followed by health plan-related issues. Both health system and health plan barriers to care jumped approximately 9 percentage points between 2003 and 2007.
Although insured people remained more likely than uninsured people to cite health system issues as reasons for access problems, uninsured people encountered especially large increases in health system-related access problems between 2003 and 2007, which accounted for most of their overall increase in access problems. For all people reporting a health-system barrier to care (see Supplementary Table 3), the greatest increases occurred for the following reasons: inability to get to the provider when the office was open (10.2 percentage point increase); inability to get through on the telephone (6.2 percentage point increase); takes too long to get to the provider (5.8 percentage point increase); and inability to obtain an appointment soon enough (4.5 percentage point increase).
Increased provider capacity constraints may have contributed to the rise in health system barriers. A shortage of some types of doctors in different markets, particularly primary care physicians, could affect people’s ability to get a timely appointment. Additionally, some physicians are becoming more entrepreneurial in response to constraints on their incomes, with responses including reducing the amount of charity care they provide and limiting their availability outside of normal business hours and over the telephone (a service that is not billable).7 Further, capacity constraints among safety net providers serving low-income and uninsured people, such as community health centers, may contribute to access problems.8 In addition, increased difficulties finding transportation, obtaining leave from work and arranging childcare are potential explanations for increased difficulties getting to providers, especially for uninsured people.
The health plan-related barriers that people increasingly cited were that their health plan would not pay for treatment (9.2 percentage point increase), followed by the doctor or hospital would not accept their insurance (4.5 percentage point increase). The return of health plan prior-authorization requirements for certain services may be a contributing factor.9 Also, rising insurance deductibles or coinsurance that cause people to be responsible for much or all of a medical bill may contribute to some people reporting that their health plan would not pay for the treatment. The increase in people reporting that their doctor would not accept their insurance may mean more doctors are opting out of private insurance networks or not accepting new Medicare or Medicaid patients.
Back to Top
Implications
![]() ollowing relative stability in access to medical care between 1997 and 2003, many Americans’ access to care deteriorated between 2003 and 2007, including low-income children and people with the greatest health care needs. Particularly striking is that access to care declined the most for people with insurance coverage—likely because of the increasing financial burden associated with out-of-pocket medical expenses. Other issues that began impacting family budgets during 2007, such as rising energy and fuel costs, the home foreclosure crisis, and an expected downturn in the economy likely contributed to growing economic anxiety that caused families to pull back on spending, including for medical care.
ollowing relative stability in access to medical care between 1997 and 2003, many Americans’ access to care deteriorated between 2003 and 2007, including low-income children and people with the greatest health care needs. Particularly striking is that access to care declined the most for people with insurance coverage—likely because of the increasing financial burden associated with out-of-pocket medical expenses. Other issues that began impacting family budgets during 2007, such as rising energy and fuel costs, the home foreclosure crisis, and an expected downturn in the economy likely contributed to growing economic anxiety that caused families to pull back on spending, including for medical care.
The sharp increase in access problems for insured people strongly suggests that the access to medical care that insurance coverage previously guaranteed is declining. Insured people are facing growing cost pressures, including higher out-of-pocket spending for care, more difficulties finding providers who will accept their insurance and renewed limits on what their insurance will cover. An alternative interpretation of these results is that as individuals are exposed to more of the costs of care, they are becoming more efficient users by delaying or forgoing care that may be of low marginal value, which is the key rationale for consumer-directed health care.
The measure of unmet need used in this study does not allow for a determination of the clinical need for care or the potential health consequences of delayed or forgone care. However, the fact that unmet need increased the most for the sickest people should cause concern, as they are the most likely to experience adverse health consequences as a result of disruptions in their medical care use.
Many state and national health reform proposals call for subsidizing the purchase of private insurance coverage, with limits on the total amount of out-of-pocket spending required by individuals and families. Identifying the appropriate threshold of out-of-pocket spending will be crucial to the success of these policies, because setting these thresholds too high may result in financial burdens that will compel individuals to put off or go without needed care.
At the same time, increases in cost-related access problems are a direct result of health care costs increasing more rapidly than incomes during the past 10 years. Employment-based private insurance premiums increased 114 percent from 1999 to 2007, while average hourly earnings increased 27 percent, leaving a gap of 6.7 percentage points per year.10 Rising costs are passed on to individuals and families in the form of higher premiums, deductibles, coinsurance and copayments for services.
The problems of cost and access are inextricably linked. Without cost containment, expanded government support for insurance coverage will have to keep pace with the trend in medical care spending to maintain affordability for individuals and families. Such increases in health care costs will be difficult for governments to sustain, especially during periods of slow or negative economic growth. To the extent that cost increases are passed on to individuals, continued declines in access to care are inevitable.
Although rising costs continue to be the dominant obstacle to access to needed care, people face growing barriers related to health care system capacity and provider accessibility. This is consistent with a perception of growing medical workforce shortages, especially among primary care practitioners, which will be difficult for policy makers to address in the short term.11 When such barriers lead to delays in needed care, people ultimately may seek care in more costly hospital emergency departments with potentially more serious conditions. Uninsured people face particular health system barriers, since growth in their numbers push against capacity constraints among safety net providers. Without resources for safety net providers to keep pace with rising demand for services, unmet needs and delayed care will likely continue to rise.
Back to Top
Notes
| 1. | Strunk, Bradley C., and Peter J. Cunningham, Trends in Americans’ Access to Needed Medical Care, 2001-2003, Tracking Report No. 10, Center for Studying Health System Change, Washington, D.C. (August 2004). |
| 2. | Cunningham, Peter J., and Jessica H. May, A Growing Hole in the Safety Net: Physician Charity Care Declines Again, Tracking Report No. 13, Center for Studying Health System Change, Washington, D.C. (March 2006); Hurley, Robert E., Laurie E. Felland and Johanna Lauer, Community Health Centers Tackle Rising Demands and Expectations, Issue Brief No. 116, Center for Studying Health System Change, Washington, D.C. (December 2007). |
| 3. | Banthin, Jessica, Peter J. Cunningham and Didem Bernard, “Financial Burden of Health Care, 2001-2004,” Health Affairs, Vol. 27, No. 1 (January/February 2008). |
| 4. | May, Jessica H., and Peter J. Cunningham, Tough Trade-offs: Medical Bills, Family Finances and Access to Care, Issue Brief No. 85, Center for Studying Health System Change, Washington, D.C. (June 2004). |
| 5. | Cohen Ross, Donna, Aleya Horn and Caryn Marks, Health Coverage for Children and Families in Medicaid and SCHIP: State Efforts Face New Hurdles, The Kaiser Commission on Medicaid and the Uninsured, Henry J. Kaiser Family Foundation (January 2008). |
| 6. | Strunk, Bradley C., Paul B. Ginsburg and John P. Cookson, “Tracking Health Care Costs: Declining Growth Trend Pauses in 2004,” Health Affairs, Web exclusive (June 21, 2005). |
| 7. | Pham, Hoangmai H., and Paul B. Ginsburg, “Unhealthy Trends: The Future of Physician Services,” Health Affairs, Vol. 26, No. 6 (November/December 2007). |
| 8. | Hurley, Felland and Lauer (December 2007). |
| 9. | Draper, Debra A., and Paul B. Ginsburg, Health Care Cost and Access Challenges Persist: Initial Findings from HSC’s 2007 Site Visits, Issue Brief No. 114, Center for Studying Health System Change, Washington, D.C. (October 2007). |
| 10. | Ginsburg, Paul B., U.S. Senate Finance Committee Testimony on Health Care Costs (June 3, 2008). |
| 11. | Colwill, Jack M., James M. Coltice and Robin L. Kruse, “Will Generalist Physician Supply Meet Demand of an Increasing and Aging Population,” Health Affairs, Web exclusive (April 29, 2008). |
Back to Top
Data Source
This Tracking Report presents findings from the HSC 2007 Health Tracking Household Survey and the Community Tracking Study Household Surveys from 1996-97 and 2003. All three telephone surveys use nationally representative samples of the civilian, noninstitutionalized population. Sample sizes include about 60,000 people for the 1996-97 survey, about 47,000 people for the 2003, and about 18,000 people for the 2007 survey. Response rates for the surveys are 65 percent in 1996-97, 57 percent in 2003 and 43 percent in 2007. Population weights adjust for probability of selection and differences in nonresponse based on age, sex, race or ethnicity, and education. Although all three surveys are nationally representative, the samples for the 1996-97 and 2003 surveys were largely clustered in 60 representative communities, while the 2007 survey was based on a stratified random sample of the nation. Standard errors account for the complex sample design of the surveys. Questionnaire design, survey administration and the question wording of all measures in this study were similar across the three surveys.
Estimates of unmet need and delayed care were based on the following two questions: (1) “During the past 12 months, was there any time when you didn’t get the medical care you needed?” and (2) “Was there any time during the past 12 months when you put off or postponed getting medical care that you thought you needed?” For those reporting either an unmet need or delayed care, follow-up questions were asked to determine why. Responses included worry about cost, problems with health insurance, problems with availability of medical providers and personal reasons, such as lack of time or procrastination. This Tracking Report includes only responses where at least one of the reasons had something to do with the health care system; responses related to personal reasons only were not considered as unmet need or delayed care. Insurance status reflects coverage on the day of the interview and includes coverage obtained through employer-sponsored and individually purchased private insurance, Medicare, Medicaid, the State Children’s Health Insurance Program (SCHIP), other state programs, TRICARE and other military insurance programs, and the Indian Health Service.
Back to Top
Supplementary Table
Supplementary Table
1: Indicators of Access to Care for the U.S. Population
Supplementary Table 2:
Reasons for Access Problems, Among People Reporting Delaying or Going Without
Needed Care
Supplementary Table 3:
Detailed Reasons for Access Problems, Among People Reporting Delaying or Going
Without Needed Care
ISSUE BRIEFS are published by the
Center for Studying Health System Change.
600 Maryland Avenue, SW, Suite 550
Washington, DC 20024-2512
Tel: (202) 484-5261
Fax: (202) 484-9258
www.hschange.org